

Investigating the molecular mechanisms underlying APOL1 kidney disease using a unique human urine-derived podocyte cellular model.
This study is with collaborators based at King’s College London
Dr Ania Kozell
https://www.kcl.ac.uk/people/ania-koziell
Dr Kate Bramham
https://www.kcl.ac.uk/people/kate-bramham
Dr Subhankar Mukhopadhyay
https://www.kcl.ac.uk/people/subhankar-mukhopadhyay
People of African descent have a 3-4 times higher risk of chronic kidney disease compared with other ethnicities. This is largely due to the presence of two common protein-altering variants in the Apolipoprotein L1 (APOL1) gene G1 and G2, found exclusively in people of African ancestry. Other populations only express the wildtype (WT) or G0 allele. (1).
Carrying a single high-risk allele (G0/G1 or G0/G2) offers protective benefits against certain infections. However, the presence of two variants, classified as a high-risk genotype (HR; G1/G1, G2/G2, G1/G2), greatly increases the risk of developing kidney disease. The underlying molecular mechanisms remain poorly understood and a “second hit” such as infection (e.g. HIV) or inflammation may be necessary.
Furthermore, APOL1 mediated kidney disease has a phenotypic spectrum, partially dependent on the presence of additional modifying exonic mutations in APOL1. Emerging data from Dr Koziell’s group also supports differences in baseline methylation as another potential mechanism. Importantly, not all HR APOL1 genotype individuals develop kidney disease and this remains unexplained.
The main target for cellular damage in APOL1 mediated nephropathy are podocytes, highly specialized epithelial terminally differentiated cells in the Bowman’s capsule of the kidney. We has developed a unique technique for growing primary podocytes from patient urine to enable study of the molecular mechanisms underpinning podocyte injury in kidney disease. Dr Koziell’s group have also gathered a unique cohort of 500 patients of African descent (APPLE-CKD) locally at KCL supporting the study and have an immortalised podocyte cell lines to verify findings.
Aims
Urine samples from G0/G0, G1/G1 and G2/G2 individuals with and without CKD will be comparatively analysed for indicator of kidney injury
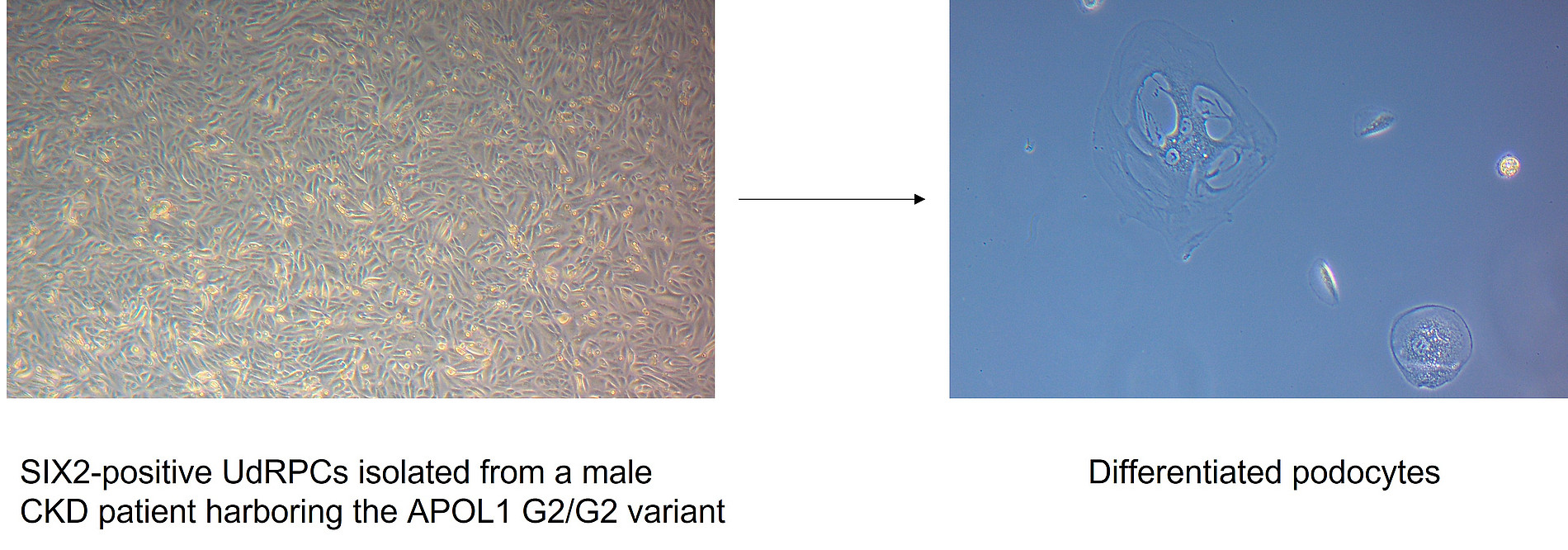
We apply our published protocol for isolating SIX2-positive UdRPCs from patient (G1/G1) and (G2/G2) urine and further derivation of iPSCs.
Comparative differentiation of UdRPCs and iPSCs into podocytes and the effect of stimulation with pro-inflammatory proteins are investigated at the molecular level
In our previous study, we used a kidney injury-specific assay to assess biomarkers in the urine of healthy individuals and CKD patients (2).

CKD biomarkers identified on the Human Kidney Biomarker Array
(A) Experiments cluster heterogeneously based on the global kidney cytokine expression.
(B) Heatmap and (C) barplot of biomarkers in males
Up-regulated: ADIPOQ, AG, ANXA5, CCN1, FABP1, IL10, LCN2 / NGAL, MMP9, RETN, SERPINA3, TNFA, TNFSF12 and VEGF
Down-regulated: AGER, AHSG, ANPEP, CLU, CXCL16, MME and RBP4.
(D) Heatmap and (E) barplot of biomarkers in females
Up-regulated: AG, AHSG, CLU, IL1RN, MME, RETN, TNFSF12 and VCAM1.
Down-regulated: ADIPOQ, AGER, ANPEP, ANXA5, CCL2, CCN1, EGFR, IL6, MMP9, PLAU and VEGF.
LCN2/NGAL and CLU are well established biomarkers of acute kidney injury/AKI and CKD
Comparative secretion of pro- and anti-inflammatory cytokines from urine derived from healthy and CKD patients

CKD-associated inflammatory biomarkers identified using a human XL cytokine assay
(A) Data cluster into CKD and healthy control based on global cytokine expression. (B) Heatmap and (C) barplot of markers in males (M) that were up-regulated (up) or down-regulated (down). (D) Heatmap and (E) barplot of markers in females (F) that were up-regulated (up) or down-regulated (down). Markers in experiment series 3 that overlapped between females (F) and males (M) that were up-regulated in CKD: APOA1 (up), ANGPT2 (up), C5 (up), CFD (up), GH1 (up), ICAM1 (up), IGFBP2 (up), IL8 (up), KLK4 (up), MMP9 (up) and SPP1 (up).
1. APOL1 Bi- and Monoallelic Variants and Chronic Kidney Disease in West Africans (2025). H3Africa Kidney Disease Research Network N Engl J Med 392:228-238
2. Wasco Wruck, Vincent Boima, Lars Erichsen, Chantelle Thimm, Theresa Koranteng, Edward Kwakyi, Sampson Antwi, Dwomoa Adu, James Adjaye (2020). Urine-Based Detection of Biomarkers Indicative of Chronic Kidney Disease in a Patient Cohort from Ghana. J Pers Med 13.